We aspire to provide compassion and hope
The Mission Cancer Foundation Patient Assistance Fund provides up to $500 of financial assistance annually to adult cancer patients undergoing medical oncology treatment in Central Iowa.
Assistance helps cover expenses including:
- Rent or mortgage
- Utilities
- Telephone
- Transportation
Donate to the Patient Assistance Fund
Your tax-deductible gift to our Patient Assistance Fund helps increase access to cancer care and ease the financial burdens that patients experience during cancer treatment. All donations stay in Central Iowa with 100% of the funds directly supporting patient and family needs.
Apply for Patient Assistance
Patients seeking financial assistance for supportive services and resources may complete the online application or request a printable copy of the application and submit it via mail, email, or fax. The Mission Cancer Foundation will review the application on a rolling deadline to approve or decline your submission. Once a determination has been made, you will be notified via email.
Step 1:
Patient qualification relies on the following eligibility criteria:
-
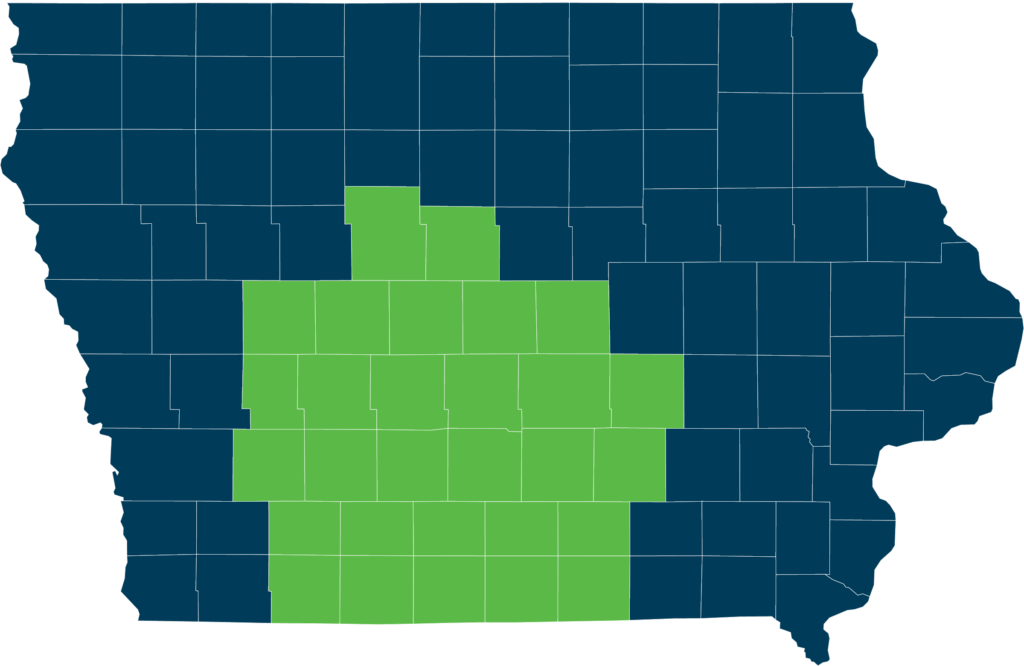
You must be receiving active medical oncology treatment in or reside in the following Central Iowa counties: Adams, Adair, Appanoose, Audubon, Boone, Carroll, Cass, Clarke, Dallas, Decatur, Greene, Guthrie, Hamilton, Jasper, Lucas, Madison, Mahaska, Marion, Marshall, Monroe, Polk, Poweshiek, Ringgold, Story, Taylor, Union, Warren, Wayne, Webster.
-
Meet annual household income requirements, 300% FPL
| # in Household | 2023 Income |
| 1 | $43,740 |
| 2 | $59,160 |
| 3 | $74,580 |
| 4 | $90,000 |
| 5 | $105,420 |
| 6 | $120,840 |
| 7 | $136,260 |
| 8 | $151,680 |
- Must have read and accepted the Grant Restrictions (located on the Patient Assistance Application)
Step 2:
Gather information needed for the application:
- Patient Information
- Financial Verification (Income Tax Return & most recent pay stub, or Social Security Award Letter if taxes not filed. If your current tax documents do not reflect your current income, please send proof of the current income, income tax return, and letter of explanation of the change.)
- Expense Verification (copies of bills needing payment assistance)
- Health Statement signed by a member of your medical care team.